In the complex world of medical terminology, understanding the differences between decorticate vs decerebrate posturing is crucial. These two conditions, although similar, have distinct implications for a patient’s health and recovery prospects. Navigating these concepts requires not only a grasp of medical facts but also a dive into the ethical and philosophical implications of life-sustaining interventions. As we explore these themes, we will see how medicine and philosophy intertwine in guiding decisions around care.
Introduction to Posturing Medical Terms
Posturing refers to involuntary flexion or extension of the arms and legs, indicative of severe brain injury. Medical professionals often distinguish between two types: decerebrate and decorticate posturing. These terms describe the body’s response to significant neurological distress, typically observed in patients with critical brain damage. Understanding these responses is vital for assessing the severity of brain injuries and determining the appropriate medical interventions.
Decerebrate Posturing Explained
Decerebrate posturing occurs when there is damage to the brainstem or upper brain regions, resulting in the arms and legs extending rigidly. This posture is typically a sign of severe brain injury and is often associated with worse outcomes than decorticate posturing. Patients displaying decerebrate posturing often have a poor prognosis due to the extensive nature of brain damage involved.
In medical assessments, recognizing decerebrate posturing is critical as it indicates a deeper level of brain dysfunction. Healthcare professionals must act swiftly to address the underlying causes and mitigate further neurological damage. Understanding the exact nature of this condition can help tailor interventions and support decision-making processes for both families and medical staff.
Decorticate vs Decerebrate: Key Differences
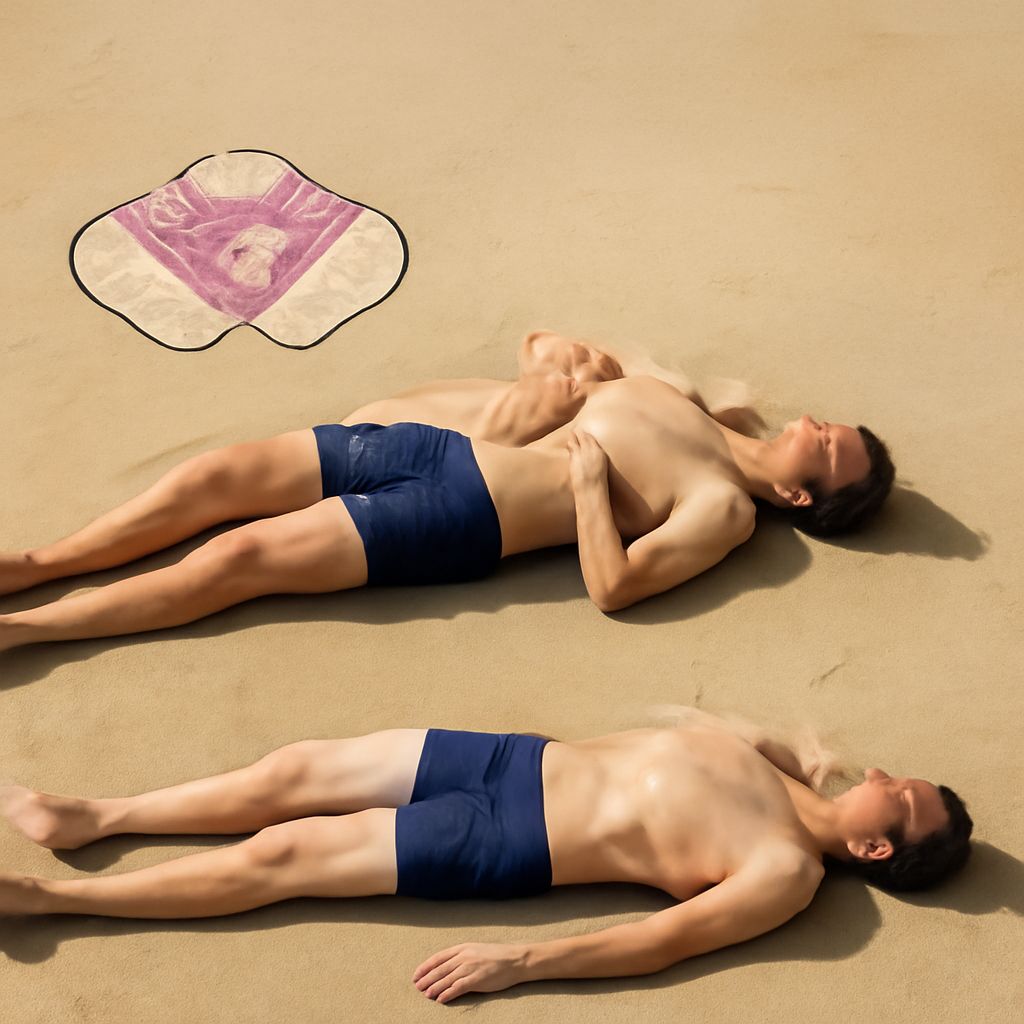
While both decerebrate and decorticate posturing indicate significant brain injuries, they differ in their presentation and underlying causes. Decorticate posturing is characterized by stiff, bent arms, clenched fists, and straight legs. This posture suggests damage to the cerebral hemispheres but less severe than decerebrate posturing. Conversely, decerebrate posturing involves extended arms and legs with the head arched backward, indicating more severe brainstem damage.
The primary distinction lies in the level of brain injury and the affected neurological pathways. Understanding these differences is crucial for medical professionals when evaluating a patient’s condition, as it directly impacts treatment strategies and prognostic discussions with families.
Ethical Considerations in Medical Posturing
The presence of decerebrate or decorticate posturing raises important ethical questions regarding patient care and the extent of medical intervention. Families and medical teams must balance the potential for recovery against the quality of life and the likelihood of prolonged suffering. These decisions often involve complex considerations, including cultural, religious, and personal values.
Ethical dilemmas often arise when deciding whether to pursue aggressive treatments or opt for palliative care. The severity of decerebrate posturing, for instance, may lead to discussions about end-of-life care and the ethical implications of prolonging life through artificial means. Here, the principles of medical ethics, including autonomy, beneficence, non-maleficence, and justice, play crucial roles in guiding these sensitive decisions.
Philosophical Reflections on Extensor Posturing
From a philosophical standpoint, extensor posturing, such as that seen in decerebrate conditions, prompts reflection on the nature of consciousness and the essence of human life. It challenges us to consider what it means to have a life worth living and how we define a meaningful existence. Philosophical discussions can offer valuable insights into the ethical frameworks that support medical decisions.
These reflections often extend to broader societal values regarding life, suffering, and medical intervention. Philosophers may debate the moral implications of sustaining life in a state of profound neurological impairment and explore how these views influence personal and collective decisions in healthcare settings.
Conclusion: Bridging Medicine and Philosophy
The exploration of decorticate vs decerebrate posturing illustrates the intersection of medical facts and philosophical inquiry. Understanding the medical underpinnings of these conditions is essential for effective treatment, but ethical and philosophical considerations provide a deeper context for decision-making. By integrating these perspectives, healthcare providers can offer more compassionate and ethically sound care to patients and their families.
Next steps: Medical practitioners and caregivers are encouraged to continue their education on neurological posturing and its implications. Staying informed about the latest research and ethical guidelines can enhance patient care and support informed decision-making. Regular training and interdisciplinary discussions can further bridge the gap between medical practice and philosophical understanding.